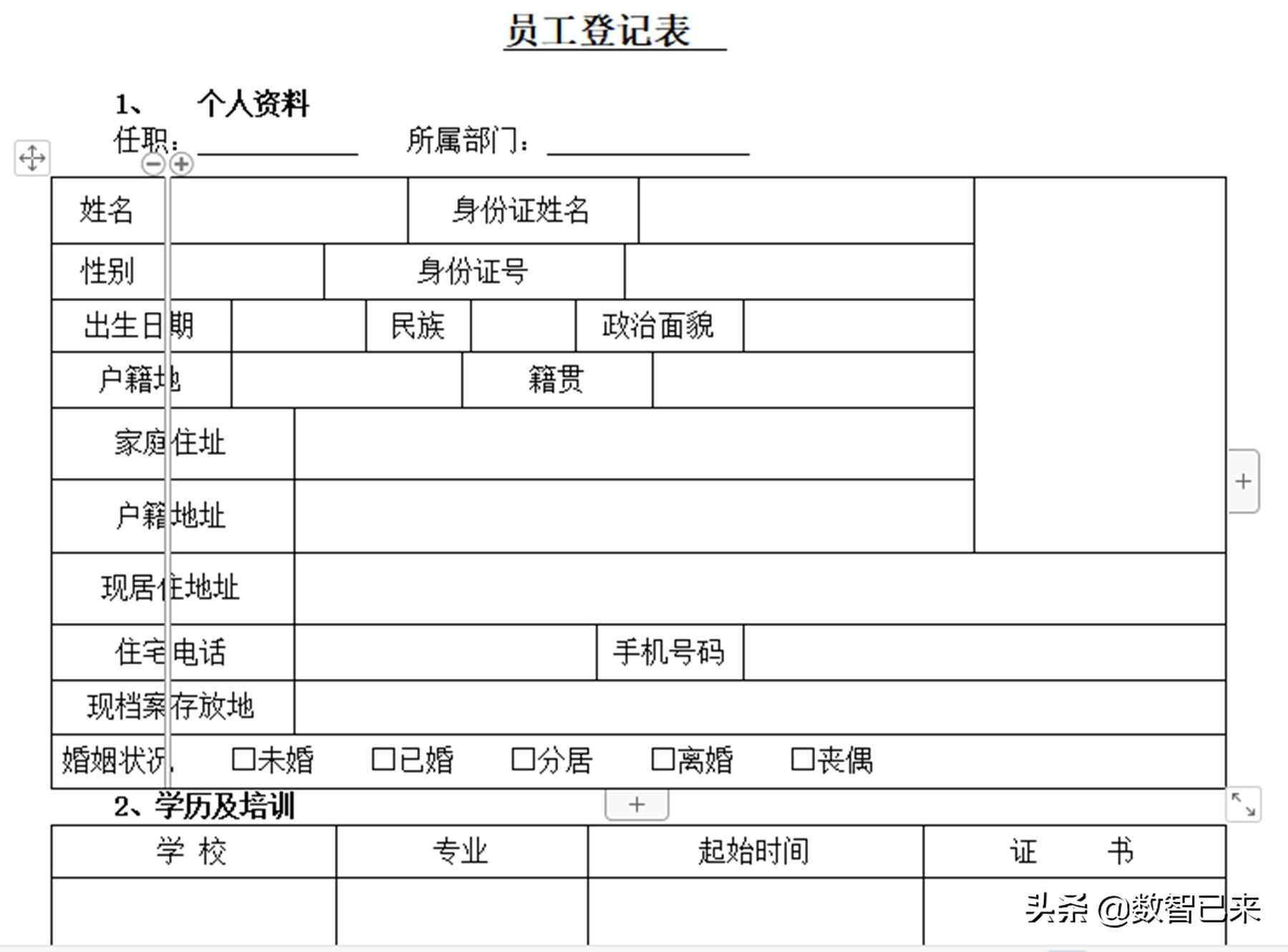
1. Personal Information
Position: Department:
Name | ID card name | ||||||||||||||
Gender | ID card number | ||||||||||||||
Date of birth | Ethnicity | Political outlook | |||||||||||||
Registration place | Place of origin | ||||||||||||||
Home address | |||||||||||||||
Household address | |||||||||||||||
Current residential address | |||||||||||||||
Residential phone number | Mobile phone number | ||||||||||||||
Current file storage location | |||||||||||||||
Marital status □Single □Married □Separated □Divorced □Widowed | |||||||||||||||
2. Educational qualifications and training
| < p style="text-align: center;" data-track="38">School | Professional | Start time | Certificate |
3. Work history
Name of the institution where you work | Position | Monthly income | Start time | Contact number | Certificate |
4. Direct family members (parents/spouse/children/siblings)
Relationship | Age | Working organization and phone number | Position | |
5. Please fill in your strengths and interests to help show your personal advantages;
.
6. Do you have anyone familiar with you in our company? If yes, please fill out the form below:
Department | Position | Relationship | Remarks | |
7. Health status
Height Weight Physical health |
If you are a woman, are you pregnant now? Yes□ No□ |
Have you ever been injured or had surgery? Yes□ No□ If yes, please explain: |
If you currently have the following symptoms, please use (a) to express and explain Yes□ No□ |
□Speech □Vision □Hearing □Intelligence □Skin disease □Lung disease □ Hepatitis □ Diabetes □ Epilepsy □ Mental illness □ Kidney disease □ Other diseases Details: |
8. Emergency contact person (this field must be filled in)
| < p style="text-align: center;" data-track="171">Name | Relationship | Address (zip code) | Landline/mobile phone |
9. Statement
I declare that the above information is completely correct and I have not deliberately concealed any facts. I have terminated the labor relationship with my original employer. Otherwise, I will be responsible for all disputes arising therefrom. I agree that if the submitted information is found to be false, the company has the right to terminate the labor relationship with me without any compensation. I allow the above information to be verified and am willing to undergo necessary physical examinations. Employee’s signature: Date: Year Month Day |
10. Please attach the following materials:
1. Copy of ID card;
2. Copies of graduation certificate and degree certificate;
3. Copies of other valid qualification certificates;
Instructions for filling out the form:
1. "Name on ID card" fill in the name on the ID card;
2. "Home address" refers to my permanent residential address in Nanjing. If there is no fixed residence in Nanjing, fill in the residential address of my parents;
3. "Household Registration Address" fill in the address where the household registration is located, based on the household registration book;
4. "Emergency contact person" please fill in the relative or friend with whom you have the closest relationship; "landline/mobile phone" needs to have both;
5. This form is an integral part of employee files and is kept by the office;
Articles are uploaded by users and are for non-commercial browsing only. Posted by: Lomu, please indicate the source: https://www.daogebangong.com/en/articles/detail/zhi-chang-yuan-gong-deng-ji-biao.html
 支付宝扫一扫
支付宝扫一扫 
评论列表(196条)
测试